International Journal of Structured Assocoation Technique No.3 pp.35-60
Original Article
Reconstructing Life and Society with SAT Therapy
: Foundations of the New Generation CBT
Tsunetsugu Munakata, Dr H Sc
President, Academy for Health Counseling
Professor & Chair, Department of Human Care Science, University of Tsukuba, D511,
1-1-1 Tennoudai, Tsukuba, Japan 305-8577 e-mail: munakata@hcs.tsukuba.ac.jp
Summary
All mammals, including humans, instinctively control through attachment behaviors their fear of not being able to subsist. Under normal circumstances, a child's principal care provider is his or her parents or guardians. However, if the latter are emotionally unstable, the child, who is supposed to be the care recipient, unwittingly becomes the one that provides the emotional care the parents or guardians covet. As a consequence, even after the child becomes an adult, he/she will unconsciously seek out an emotionally unstable family member or colleague at work and build a codependent attachment relationship replacing the former parent-child relationship in which one relies on the other and vice a versa. Such relationships, however, create a whirlpool of undue stress accompanied by "insecurity, distrust and exploitation." To be able to overcome subsistence fear and build a stable attachment relationship marked by "ease, respect and gratitude," the individual needs to change the facial expressions and images of "tension and irritability" he/she remembers of their parents or guardians to those of "smile and serenity."
SAT is a structured imagery therapy used to promote reconstruction of stable attachment relations through the application of a subjunctive mood that takes clients back through evolutionary time to their ancestors and ultimately to their particles. A certified SAT therapist uses a retrospective image projection technique, including pictures, paintings, religious paintings, and comic books, to help clients discover their parental surrogate representations. By having clients observe these parental surrogate representations instead of the expressions and images of their actual parents or guardians, the SAT therapist helps clients reduce their negative emotions, thereby helping them to break up their codependent attachment relationships. SAT therapy is thus a new-generation CBT (cognitive behavioral therapy) that promotes rational thinking compatible with the client's genetic disposition.
Keywords:
attachment, codependency, parental surrogate representation, cognitive behavioral therapy, SAT therapy
Introduction
Since ancient times, society has been organized in such a way that people have to rely on others to gain access to scarce rewards. In such a society (hereinafter referred to as "other-reward-seeking society), people have to compete or fight with each other to gain access to scarce rewards such as evaluation, praise, honor, income and status. In an other-reward-seeking society, people cannot help but be stressed out. But what if we could build a society where people help each other to gain access to unlimited rewards such as self-growth, self-satisfaction, gratitude, empathy, inspiration, pleasure and sense of accomplishment. Even in such a society (hereinafter referred to as "self-reward-seeking society") people will still be under stress, but stress here would be benign enough to allow people to learn from their mistakes and develop a genuine sense of well-being. According to surveys conducted by the Cabinet Office, since the 1980s, the tendency of Japanese to seek richness of mind, such as spiritual growth, gratitude and inspiration, rather than material affluence has increased significantly over the passed 30 years. Indeed, expectations have heightened for the creation of a self-reward-seeking society.
However, in a traditional other-reward-seeking society, where people have to rely on others to gain access to limited resources, top priority is put on social adaptation. Consequently, from our early childhood, parents and guardians, in the name of discipline, refuse to let us "just be ourselves," and subject us, to a greater or lesser extent, to emotional and physical abuse that conditions us to physical fear. Thus we are afraid to express "our true selves," which inherently lie deep in our hearts. We are unable to change, even if we wanted to. As our self-conflict deepens and our malignant stress intensifies, our stress disorder continues to expand. However, it can also be said that as our stress disorder continues to expand, we are actually accumulating energy for self-growth. In order to realize a self-reward-seeking society where people can universally experience a sense of well-being by realizing their "true selves," in this paper I would like to take up the theory of SAT therapy, along with its methodology, as a form of cognitive behavioral therapy that will help clients solve their unresolved issues over codependency attachment relations, which will enable them to survive in an other-reward-seeking society.
In recent years, cognitive behavioral therapy (CBT) has been applied to help people change their thinking habits from those that cause them to suffer malignant stress to those that are more adaptive to their situation. However, while it is true that CBT has helped people change their thinking habits in the short-term by making changes that, on paper, appear rational, CBT may also lead to somatization and acting out of stress. This is because, when the forebrain, (which is involved with reasoning) and the limbic brain (which is involved with emotions) are in opposition, the latter trumps the former. This is why a new generation of cognitive behavioral therapy is needed that will not only change our thinking habits but also directly alters our emotions.
1. Attachment is indispensable for life
Attachment runting syndrome
A runt - the smallest and weakest animal of a litter - will die a few weeks after birth even when no change has occurred in the environment. This is because the runt is too weak to stimulate the mother's nipple for milk and induce her to engage in the attachment behavior associated with grooming. A form of human bonding called attachment is formed between a mother and a child via oxytocin secretion not only at the time of delivery but when there is physical contact including when the baby suckles. Unless this attachment bond is formed, the mother will be less and less inclined to give the runt physical care such as grooming. As a result of this neglect, the runt will experience so much stress that it becomes difficult for its body to secrete growth hormones. The same thing occurs in human offspring as evidenced by the fact that many children in orphanages have been reported to suffer from a low level of a growth hormone known as nonorganic hypogenesis (Stanhope et al., 1994; Albanese et al., 1994). These runting syndrome cases demonstrate the importance of getting parents and guardians to engage in attachment behavior to control subsistence stress and ensure survival.
That said, I think forming a stable attachment relationship after birth requires almost a miracle. Of course, trying to make that miracle happen may be admirable, but it is better to take the view that each client has an attachment relationship suited for him or her situation. Nevertheless, depending on the nature of the attachment relationship formed, the client will in some cases end up leading an unexpectedly complicated life.
What Is Attachment?
Johan Bowlby (1969) named the "emotional bond" formed between mother and child "attachment," arguing that even infants inherently seek to form proximity relationships with selected targets. In other words, to gain their affection, infants behave in a way that will bring them closer to their caregivers. There are a number of attachment behavioral patterns that are formed in this process. According to the famous technique for measuring the quality of attachment that Mary Ainsworth (1978) developed by applying her Strange Situation method, there are four types of attachment patterns: "avoidant attachment," "secure attachment," ambivalent attachment" and "disorganized attachment." Attachment behavior is "behavior that seeks to gain a sense of security in time of fear by drawing the caregiver's attention and seeking proximity. By repeating this behavior, the infant is assured that the caregiver will provide protection, thereby enhancing its ability to cope with stress.
Roundabout way of forming attachments
What happens to children when their parents or guardians mentally and physically reject them by refusing to accept them "as they are" and are thus subjected to such severe emotional and physical abuse that they are unable to form safe and secure attachment relations with their parents or guardians?
First of all, they will show behavioral patterns in which they personally try to void attachments out of feeling of dread. Being suspicious of caregivers they encounter, they might show self--repressive behaviors, that is, behavior patterns in which they try to suppress their longing to be looked after by their parents or guardians. They do this because they have developed a sense of caution in their past relationships with their parents or guardians, and have transplanted these unstable attachment relationships to their other relationships. In extreme cases of avoidant attachment, fearful of being rejected by their caregivers, and out of a sense of caution, children develop a belief that they should not turn to their caregivers for help and so unconsciously begin to suppress their longing for care. These children then begin to show alexithymia behaviors in which they try not to show any emotions and work very hard to do things by themselves.
When parents or guardians refuse to accept children as they are, the latter may also show problem-avoidance behaviors that cause them to act independently and become insensitive to their own problems. They may also show problem-avoidance behaviors that compel them to act as if their problems were not really theirs, and show depersonalized behaviors in which, instead of relying on their parents or guardians to give them care, they turn to themselves. Because of these behaviors, children become insensitive to tensions associated with stress and continue to accumulate such more stress that they manifest physical disorders, which in turn lead to stress disorders and diseases associated with adult lifestyle (Munakata, 2004, 2006; Munakata, Kobayashi, 2007). But these can be regarded as illness behaviors that seek attachments in a roundabout way by drawing the attention of caregivers and promoting formation of proximity relationships.
Children who fail to form legitimate attachment relationships not only distrust others but also become more inclined to deepen their sense of self-denial, thus driving them to seek care from caregivers in a distorted manner known as parasuicide, which includes cutting one's wrist, planning to commit suicide, and increasing accident proneness. Or, because of their inability to trust others, they refuse to rely on people's kindness and end up developing substance dependence on alcohol, drugs and the like that affect their psychoneurotic system.
2. Trauma dependency syndrome and codependency bond
Trauma dependency
I'm sure most of you have heard the term "runner's high." Human beings possess a stress reaction system that discharges a chemical substance called endorphin in the brain to relieve pain and bring comfort when they find themselves in a highly stressful, life-threatening situation (Perry & Szalavitz, 2006). Those with a traumatic experience of being powerless in the face of life-threatening danger to themselves or to others have experienced being in a highly stressful situation where a chemical substance is discharged in the brain to relieve pain and bring comfort. This is why when those with serious traumatic experiences are delivered from their high levels of stress, they develop a sense of irritability, fear, excess arousal and feeling of helplessness not unlike the symptoms addicts experience when they stop taking morphemes or heroine. However, because trauma patients do not suffer the same withdrawal symptoms as drug addicts do, they compulsively seek even higher levels of stress. Consequently, they become more inclined to become addicted to trauma (Van der Kolk & Greenberg, 1987).
Children with serious traumatic experiences can't bear being in a quiet place. They are prone to risk-taking behaviors like fighting, bullying, gang warfare, delinquency, wrist cutting, accident proneness, depression and suicide attempts, as well as tobacco, alcohol and drug dependency. They avoid quiet atmospheres, draw the attention of caregivers by acting precariously, and try to stay attached to them by forming proximity relationships. In addition, at least physiologically, they maintain the highly stressful condition they're in and retain the high level of endorphin secretion in their brain in order to overcome their irritability, sense of fear, and feeling of helplessness.
Trauma-bonding
Out of fear or disgust, children who have been sexually abused by their fathers may be expected to be completely repulsed by sex. But contrary to such expectation, sexual abused trauma survivors tend to engage in promiscuous sexual behavior even with complete strangers (e.g., fellatio). They engage in such acts not as an expression of affection, but rather as an "act of submission." By acting this way, survivors of childhood sexual abuse learn that adults who are potentially dangerous may not turn out to be their worst enemy.
The following behavioral pattern is generally observed among many Japanese. Trauma survivors raised by physically abusive fathers and mothers who refused to come to their rescue tend to engage in self--repressive behavior known as "act of submission" in which they send strong authority figures expressive messages in the form of facial, voice, and bodily movements to let them know how harmless and submissive they are, thereby leaving a favorable impression on the other party.
Because they experienced relationships based on fear, survivors of childhood traumatic experiences such as sexual abuse, abusive upbringing, and neglect are unable to form stable attachment relationships based on an original sense of reassurance. As a result, they form distorted codependency relationships (both dependency they want for themselves and dependency they want to force on others) known as trauma-bonding that goes beyond social convention. Trauma victims tend to form codependency relationships with other trauma victims. Perhaps, they do this because, on a gut level, they feel they cannot form such relationships with anyone who does not have similar traumatic experiences. In other words, based on the expressive messages of caregivers conveyed in the form of facial expression, voice and bodily movement, trauma victims, as members of the disadvantaged, on a gut level, foresee receiving care from caregivers who are themselves trauma victims. They feel in their bones that such caregivers will without a doubt rescue the disadvantaged, and in the process they come to know intuitively how to exploit their caregivers to their advantage. Since caregivers who are themselves trauma victims can gain self--satisfaction or be rewarded in the form of being healed by having the underdog trauma victims become depended on them, the latter anticipate that caregivers will come to rescue them, just as drug addicts seek relief by turning to drug dealers.
Although the act of one trauma victim rescuing another trauma victim may appear altruistic, the former is actually rescuing himself. His is a narcissistic behavior. When a rescuer rescues a person who is disadvantaged in order to rescue himself, he is doing this only to satisfy himself. Thus, when such a rescuer is unable to get satisfaction, the person who is supposed to be rescued is not rescued; instead, he is more likely to be betrayed. Regardless whether relationships are based on social functions - such as those between husband and wife, parent and child, and master and pupil - or therapeutic relationships, as long as they are codependency relationships, those with traumatic experiences, because they are disadvantaged, may, upon seeing the expression of the disadvantaged, react by trying to rescue the disadvantaged. However, caregivers who are supposed to rescue trauma victims from their sufferings, because they cannot get satisfaction themselves, are apt to turn into trauma caregivers who are apt to be a source of fear and sufferings for trauma survivors.
If trauma survivors are able to form only distorted attachment relationships dominated by fear, they may develop Munchausen syndrome, which forces patients to draw attention of caregivers to themselves in the hope of forming proximity relationships with them by engaging in parasuicidal behaviors, or they may develop Munchausen syndrome by proxy, a variant of Munchausen syndrome, that forces them to draw attention of those around them and form proximity relationships with them by caring for children or adults who have experienced tragedy. A person affected with Munchausen syndrome in proxy ensures that her child will become ill, thereby forcing the child to take tests and undergo treatments that are not really necessary. While the affected person takes care of the child, those around her direct their concerned look toward her and begin to hug her as a sign of encouragement. This response is precisely what the affected person seeks.
According to past studies of Munchausen syndrome in proxy, patients with serious symptoms may experience tragic consequences. In one study, the researchers recorded on video the behaviors of 39 mothers apparently afflicted with this disorder. When the video was shown, one of the mothers actually confessed to killing her child (Southall et al., 1997). In Japan, Europe and the U.S., there are cases where nurses and other caregivers, possibly with Munchausen syndrome in proxy, have driven patients to tragic ends.
While those afflicted with codependency pathology may commit the most heinous acts of tyranny imaginable, it is also true that, as they wander astray, they may be observed performing the most beautiful acts of kindness humans are capable of performing (Perry & Szalavitz, 2006). In my view, trauma victims can only be rescued by trauma victims. Only those who have experienced traumatic events themselves will stay around those with trauma dependency syndrome. Whether they are husband and wife, parent and child, master and pupil, or in therapeutic relationships, they are expected to overcome their anxiety, distrust and exploitation of the codependency type of attachment relationships and in the process establish stable attachment relationships of reassurances, respect and gratitude. Toward this end, it is necessary for both parties to become aware of their mutual longing for codependency.
3. How to overcome codependency
Other-reward-seeking behavior and self-reward-seeking behavior
Although there are individual differences, children are usually motivated to act in ways that will reinforce the reward responses in which the expressions and images of the faces, voice and bodily movements of their parents or guardians express "happiness." Or they may be motivated to avoid responses of revulsion that express the doubt, anger and sadness of their parents or guardians. In other words, children choose behaviors that reinforce the formation of attachments. Even when they become parents or guardians, themselves, they are motivated by the reward responses of their significant others in social groups like school, society, and post-marriage families, resulting in the formation of other-reward-seeking behaviors that help reinforce attachments.
On the other hand, from our childhood days, it is through self-reward-seeking responses, such as solitary play, playing with friends, adventure, art and sports activities, and caring for plants and animals, that we can enjoy ourselves and become motivated to act in ways that will reinforce these responses These responses help increase our sense of self- trust and enable us to develop into mature individuals capable of controlling the countless stressors we encounter in life. These motivations enable us to form self--reward-seeking behaviors after we mature into adults.
Since other-reward-seeking behaviors conform to the evaluation of others for forming attachments, it is easy to avail oneself to the resources of others. That said, it is others who possess positive resources - e.g., praise, favorable impression, repayment, honor, status, income - and negative resources - e.g., threat, punishment, restraint, disregard, discrimination, indifference. Consequently, with other-reward-seeking behavior one is easily swayed by the evaluation of others, which is often accompanied by tension and insecure feeling, resulting in accumulation of even more stress. Also, since other-reward-seeking behaviors require the evaluation of others, those who engage in them are apt to suppress their true feelings, thus resulting in self- denial and further aggravation of their depression.
By contrast, in the case of self-reward-seeking behaviors, it is difficult to get rewards from others but easy to give rewards to oneself - rewards like pleasure, interest, inspiration, resolve, sense of accomplishment, growth, self-satisfaction, gratitude and empathy. Since you yourself possess the resources involved in self-reward-seeking behaviors, self-rewards are easy to get, provided you are able to learn from your mistakes. This is why self-reward-seeking behaviors do not lead to accumulation of stress as with other-reward-seeking behaviors.
People cannot tell between Self and Others - Mirror Neurons
If you have experienced physical trauma in the form of emotional and physical abuse, you will be too afraid to take up self-reward-seeking behaviors, and will likely be frightened, anxious, harbor a sense of guilt, resignation, and so on, and as a result, you will not be able to act appropriately. You need to become aware that emotions such as fear, anxiety and sense of guilt are conditioned by the fear written on the expressions of your parents or guardians constituting the trauma they have experienced.
The areas of the brain that are activated differ in accordance with the difference in the expression of revulsion people make. In either case, it is now clear that, through the mediation of mirror neurons, the same location of the brain is activated in both the person making the expression and the person looking at the expression (Carter, 1998). In other words, when we look at the expression of revulsion in the faces of others, we end up having the same feeling of revulsion. If the relationship with parents or guardians is such that if we are always looking at the expression of revulsion on the face of others, the expression on our face will also become expression of revulsion. This is why children who grow up looking at expressions of revulsion on the faces of their parents or guardians find themselves making similar expressions.
How will your body react when you look at the picture below of a woman with an expression of revulsion (Fig. 1)? You might feel stiff in the shoulder. Your heart might start pounding. You might have difficulty breathing. Your hands and feet might start feeling cold. Your whole body might stiffen. How will you react if the person in Figure 1 were living next to you? How would you feel? What kind of body sensation will you have? What about your facial expression?
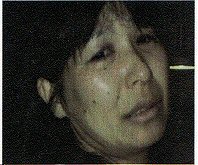

Fig. 1 Woman with an expression of revulsion Fig 2. Family with a smile
How about when you look at smiling faces those in Figure 2? What about your body sensation? And what kind of expression will you have on your face? For no apparent reason, you can feel yourself beginning to smile, can't you? This is the effect mirror neurons may have. In other words, your self-image is created by the image you have of your parents or guardians.
When your mother has a fight with her mother-in-law or with your father and mother is attacked by father, and mother looks sad like the woman in Figure 1, the mirror neurons of their children will show the same kind of excitement as their mother's emotions. From then on, for the children, the mother becomes someone they have to protect. The only way they can now form attachments with their mother is by protecting her. And the mother ceases to be a "parent" with whom they can form attachment relationships and a "parent" who will give them comfort and sense of stability. In a word, they can no longer expect their mother to look after them. This is a form of emotional neglect. To remain attached to such a mother, the children are compelled to form a self- image that seeks rewards from others. Unable to seek help from others, they have difficulty recognizing other people's feelings. Excessive positive thinking makes them avoid facing problems. They show a sympathetic nervous tone characterized by self- dissociation, which compels them to constantly watch over themselves.
When boys mature into adults and find codependent partners who resemble their mothers, they find them endearing and develop an illusion that they are in love with them. By contrast, girls grow up to become mothers closely resembling their own mothers and find codependent partners who are apt to act violently toward them.
On the other hand, how do children relate to their fathers? If they're the type who seek attachments with their father even as they revolt against him for reproaching their mother, their mirror neurons, empathizing with the father, will try to develop an other-reward-seeking type of self with whom their father will feel comfortable and safe. From then on, for the children, the father becomes someone they have to protect. The only way they can form attachments with their father is by protecting him, and from that moment, the father ceases to be a "parent" with whom the children can form attachment relationships that provide comfort and sense of stability, and the children can no longer expect their father to look after them. This too is a form of emotional neglect. Moreover, if a boy tries to protect his mother, the father will verbally or physically attack him. By being emotionally and physically abused in this manner, the boy will grow up not having formed any other father image than that of his abusive father, with the result that he will end up being just like his father, or find a partner who is obedient just like his mother. This is how the codependent attachment relationships are handed down from generation to generation.
Self-image can be changed by a proxy image of parents or guardians
Those who have a positive self-image with a strong sense of self-affirmation tend to be self- confident and are likely to anticipate that their future will open up for them. Thus they are free of anxiety and full of hope. They are proud of their past and filled with gratitude. Also, they have no regrets, are patient, free of uncertainty and depression. They have excellent mental health.
By contrast, those who have a negative self-image with a strong sense of self-denial always tend to expect the worst about their future. They easily harbor fear, anger and sadness, and therefore are unable to gain a sense of well-being. Individuals like this have a self-image marked by self-repressiveness that can be thought of as attachment relationships that bring neither comfort nor sense of stability (repressing the self to gain recognition of those around you), difficulty with emotion recognition (working hard without relying on the help of those around you), self-disassociation (maintaining composure by regarding your problem as somebody else's problem), and problem avoidance (coping with a particular situation ignoring the underlying problem and with undue positive thinking). It has become clear that, in all cases, the more pronounced these traits characterize the self-image of an individual, the more severe his or her depression gets (Munakata, 2003: 2004).
As noted above, the self-image of a client is likely to correlate with the image of his or her parents or guardians. That is to say, those who have a bad image of their father or mother also have a bad self-image and lack a sense of well-being. For example, it is now clear that those who remember their parents having an expression of revulsion like the facial expression on the woman in Figure 1 tend to have such physical symptoms as headache, stiff shoulder, lower-back pain and allergy, and have a deeply repulsive self-image, and lack a sense of well-being (Munakata, 2009).
SAT therapy
In SAT therapy, the counselor applies a subjunctive mood* to determine what would happen if a client is taken back through evolutionary time to their ancestors and ultimately to his or her particles, and as a result, the client's past is changed in a way that improves the client's own life situation. A retrospective image projection technique is applied to help the client visualize his or her parents or guardians as people who provide care unconditionally. On the basis of this image, the client discovers his or her parental surrogate representation in photographs, paintings, religious (Buddhist) paintings and bronze statues that resemble the image the client originally had of his or her parents or guardians. The client is instructed to continue looking at the parental surrogate representation so that the brain will receive visual stimulations frequently enough that they will become firmly fixed in his or her brain. Instead of looking at the facial expressions of his or her actual parents or guardians, everyday the client looks at the parental surrogate representation in photographs, paintings, religious icons, comics and the like that have the same facial expressions as the ones the client imagines his or her true parents or guardians have. Forming an attachment relationship with the improved parental surrogate representation helps the client feel better and more refreshed, which in turn enables his or her body to relax. The brain is easily affected by mirror neurons, and this is especially prominent in facial expressions. By imagining the facial expressions of his or her parents or guardians to be like those of persons who provide care unconditionally, the client is able to improve his or her self-image to resemble the smiling faces shown in Figure 2. In this way, the client learns to fix in his or her mind those smiling facial expressions as the self-reward-seeking type of self-imaging script (Munakata, 2009). Of course, together with raising his or her expectations for self-growth, the client seeks further improvement of his or her self-image, which in turn may inspire the client to come up with an upgraded version of the substitution expressions and images that he or she had already decided on.
* Note:
The retrospective journey through time covers the entire evolutionary process ranging from the Big Bang to particles to atomic nuclei to atomic elements to molecules to proteins to living organisms, and to humans. In this journey, the client is guided to recall up to the time of his or her ancestors, and through his or her parents or guidance, to his or her own births and growth. The client is then taken back to any one of the earlier evolutionary stages, where he or she improves the image of his or her parents or guardians, and in turn improves his own self-image script. Below are four ways of rewriting one's self-image script:
- Re-resolving imagery therapy: This is a technique for supporting clients' efforts to change their present self-image script by counseling them to re-learn how to solve unresolved problems dating back to their childhood days and thereby also changing the self-image script of their parents or guardians.
- Three-generation script imagery therapy (formerly, rebirth and re-rearing therapy): This is a technique for supporting clients' efforts to change their present self-image script by altering the image script they have had of their parents or guardians by urging them to go back three generations to re-resolve the crisis in the womb recalled during the womb-regression therapy.
- Pre-generation retrospective imagery therapy: This is a technique for guiding clients to change their present self-image script by altering the image script of their parents and guardians by urging them to go back in time to re-resolve the survival crisis of previous generations recalled during the womb retrogression therapy.
- Retrospective evolution imagery therapy: This is a technique for guiding clients to change their present self-image script by urging them to go back through time to re-revolve the crisis of their particles or biological existence recalled during the womb regression therapy.
Controlling the fear of human relationships
We alternate between hope and fear as we watch television and movies. It's as though we were talking with our past. We project and fear those characters in stories we ourselves have experienced in our past, and relive the anxiety, sadness and other emotions that we experienced then. Similarly, among those we have encountered since infancy, most of the others who make us feel stressed have some of the same expressions that our parents or guardians who made us feel stressed in the past had. This is why we relive the same stress. We respond to some of those expressions in the same emotional way. To explain this phenomenon, it will be useful to give yourself the test described below.
Picture in your mind the good expressions and expressions of revulsion of either your father or mother, and see how your body reacts to the expressions and images you've recalled. If the parent you recall has a good expression, of course, your body will relax, but if the parent has an expression of revulsion, your body will respond in a variety of ways: I feel tense in some parts of your body. I feel a knot of pain in my head; I feel stiff in the shoulders; I have a pain in my chest; my heart starts pounding; my stomach feels funny; my hands and feet feel cold; and my whole body becomes rigid.
Now, consider how a client's body might react if the counselor asked him or her to recall the expression on the face of a person who made him or her feel stressed. If the client were properly guided in this, you would be surprised at the expression of revulsion on the face of either the aforementioned father or that of the mother, or at the similarity of the body's responses when the client looked at the expression of both the father and the mother (Munakata, 2009).
Until the client becomes self-reliant, it is understandable that the therapist should try to control the client's survival fears by controlling the attachment relationship between the client and his or her parents or guardians. But there is no reason to fear one's parents or guardians or to be saddened after becoming independent. If you can control this fear by applying the proxy expressions and images of your parents or guardians, by all means, use them to your advantage.
Cutting the umbilical cord of codependency with SKP surrogate representation
However, there are cases where you cannot reduce your own stress merely with the parental surrogate representation. Many symptoms, like suicide attempt, alcohol/substance abuse, personality disorder, and mental illness that you cannot control acting on your own will, cannot be explained by what psychoanalytic theories (including Bowlby's theory) refer to as the way you were conditioned by your parents or guardians in your infancy. This is because there are many cases where people find happiness despite their parents' or guardians' failure to raise or condition them properly in their infancy. This is why treatment strategies (attachment therapy, play therapy) that focus only on conditioning rarely lead to cure. Such treatment strategies are more likely to lead to a pathological condition of codependency of care providers. I believe the reason these symptomatic behaviors cannot be controlled by you acting on your own is that they have their origin in the fear that conditions you during the period between the embryo and the fetus.
The first factor to consider in analyzing the period when you are still in your mother's womb is the significant effect emissions of various chemical substances (e.g., noradrenalin, stress hormones) have on the embryo and fetus that reflects the relation nature of your mother and father.
Another factor is the possibility of embryonic and fetal deaths in multiple births. Medical research has shown that only one in three zygotes test positive when urinalyses are administered on pregnant women, the rest (i.e., two-thirds) die and disappear. Although most miscarriages are caused by abnormality of chromosome, since other causes of miscarriages (i.e., half of the genetic material contained in the blastocyst) are inherited from the father, the mother's immune system regards them as viruses and attacks them, thus resulting in fetal deaths - The chemical material that remains after the remains of the dead fetuses is reabsorbed by the mother. The information carried by the reabsorbed chemical material may be stored in the cell membranes of more than 50,000 uterine cell receptors.
In the case of unborn babies of multiple conceptions, it may be that fear, anger, sense of grief and other emotions felt by the "siblings that died" are transmitted to the "siblings that survived" via their mirror neurons. This is why may be there is the possession of emotional information of our other siblings. Even if a client strongly desires to live, if the death wish, fear and sense of grief of his or her siblings have been transmitted to the client, then the client will bear a baby with contradictory emotions and personalities.
Clinical cases using SAT imagery therapy make it clear that patients with these contradictory personalities engage in destructive behaviors like attempted suicide and alcohol/substance abuse and suffer from personality disorders and mental illness. These disorders are considered to be purely diseases of the body. However, our research demonstrates that even those suffering from autoimmune diseases have similar backgrounds (Munakata, 2005; Munakata, 2007; Munakata, Kobayashi, 2007).
This is why it is necessary to devise a treatment program that will cut off the transmission of emotions afflicting the client's deceased siblings. In SAT therapy, a three-generation retro narrative imagery technique is used to trace the crisis that have fallen on the client's three generations - parents, siblings and children - by having him or her go back three generations and re-resolve the crisis in the womb recalled during the womb-regression therapy, thereby liberating itself- from his or her subconscious control by turning his or her facial expression into proxy expressions and images.
Of the three-generation family, including those "siblings that died an absurd death (miscarriage, still birth, death by accident, death by disease, etc.), "those who protect us, or those with whom we wish to form codependency relationships" are referred to as spiritual key persons (SKP). By consciously visualizing the surrogate representation of the expressions on the faces of SKPs, clients undergoing the womb-regression therapy are clearly able to feel at ease and form a tension-free self-image.
If a client does not have the necessary SKP surrogate representation, the counselor will guide him or her to seek "a person who will protect him or her, or a person he or she would like to protect" and form a codependency relationship in which the client plays the role of the underdog or the caregiver. The client is guided this way because the codependency relationship will reproduce a whirlpool of malignant stress that in turn will produce stress-ridden patients and create intractable problems. Consequently, if the client continues to look at his or her parental or SKP surrogate representation, he/she will be able to proceed to form a secure attachment relationship based on sense of ease, respect and gratitude. And if the client's parents or guardians are still alive, the latter will now be able to change his or her relationship with his or her real parents or guardians.
Conclusion
Other-reward-seeking society where people fight over limited resources, which generate a lot of malignant stress that systematically batters the very social fiber, is about to outlive its usefulness. The time has come to build a self-reward-seeking society marked by a highly-organized structure where people cooperate with each other to gain unlimited self-rewards such as self-growth, self-satisfaction and gratitude. To build such a society, we must move beyond conventional codependency relationships and form secure attachment relationships based on sense of ease, respect and gratitude.
References
- Ainsworth, M (1979). Infant-mother attachment. American Psychology 34, 932-937.
- Albanese, A, Hamill, G, Jones, J, Skuse, D, Matthew, D R, Stanhope, R (1994). Reversity of physiological growth hormone secretion with psychosocial dwarfism. Clinical Endocrinology 40(5), 687-692.
- Bowlby, J (1998). A secure base: parent-child attachment and healthy human development. Basic Books, NY.
- Bowlby, J (1982). Attachment. Basic Books Inc, NY.
- Carter, R (1998). Mapping the mind. The Orion Publishing Group Ltd.
- Munakata, T (2003). Depression as human professionals. Journal of Psychiatric and Consultation Liaison Nursing 4(1),7-13 (in Japanese).
- Munakata, T (ed.) ( 2004). Counseling Health Care, 1-272. Tokyo: Kaneko publishing company, (in Japanese).
- Munakata, T (2006). SAT Therapy, 1-24. Tokyo: Kaneko publishing company, (in Japanese).
- Munakata, T & Kobayashi, K (2007). SAT therapy for treating cancer, 1-226. Tokyo: Sinjusha, (in Japanese)
- Munakata, T (2008). Does SAT re-scripting expression imagery enable us to overcome unendurable hardships toward true life career? Journal of Health Counseling 15, 75-92 (in Japanese).
- Perry, B, Szalavitz, M (2006). The boy who was raised as a dog and other stories from a child psychiatrist's notebook. Perseus Books, Inc., Cambridge, Massachusetts.
- Rizzolatti, G, Craighero, L (2004). The mirror-neuron system. Annual Review of neuroscience 27, 169-92.
- Stanhope, R, Wilks, Z, Hamill, G (1994). Failure to grow: lack of food or lack of love? Professional Care of the Mother and Child 4(8), 234-237.
- Southall, D P, Plunkett, M C, Banks, M W, Falkov, AF, Samuels, M P (1997). Covert video recordings of life- threatening child abuse: lesions for child protection. Pediatrics 100(5), 735-760.
- Van der Kolk, B A (ed.) (1987). Psychological trauma. Washington DC.
- Van der Kolk, B A (1989). The compulsion to repeat the trauma: repeat the trauma: reenactment, revictimization and masochism. Psychiatric Clinics of North America Vol 12. Treatment of Victims of Sexual Abuse, W B Saunders, Philadelphia.